DESIGNING FOR EMOTIONAL SAFETY IN MATERNAL HEALTHCARE
Team: Lead Qualitative Researcher (me), 2 Junior Researchers, Pl
Domain: Healthcare UX, Service Design, Equity-Centered Research
Timeline: 12 months
Problem Statement
There are many factors that affect overall maternal healthcare user experience, namely negative clinical encounters with and a mistrust of providers. From a UX research perspective, there is a misalignment between user needs and system design, where healthcare environments unintentionally discourage vulnerability and help-seeking, particularly for Black women.
Many women experience a hidden system constraint that shapes how they interpret clinical encounters, regulate emotional expression, and decide whether to seek or withhold care.
project overview
study goals
Identify key pain points and barriers Black mothers face when navigating maternal healthcare systems.
Understand how mothers define a high-quality care experience and what drives trust and engagement.
Examine how expectations of strength shape user behavior and identify care models that support emotional satety.
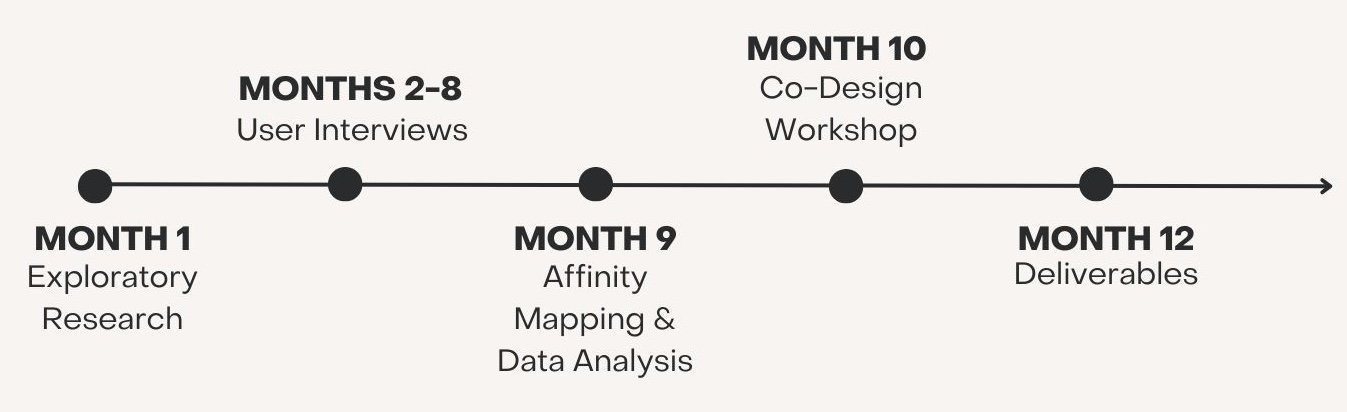
Project Timeline
User Interviews
I conducted user interviews with 30 Black postpartum (2 months) mothers to evaluate their postpartum and clinical visits, emotional and physical recovery, and how they used high-stake decisions involving pain, mental health, and support needs.
Some of our key constraints were:
Users are navigating care environments shaped by racialized expectations that reward emotional restraint and penalize vulnerability.
Users feel pressure to appear strong and capable in order to avoid judgment or dismissal from providers.
Findings
Insight: Black mothers often suppress pain, emotions, and care requests to avoid judgment or dismissal.
"I just always feel like I don't want to bother anybody, or I don't want to be a burden, or I just don't want to have to ask somebody to help me if they don't have anything to do with it.. I just wish it was a more natural thing for me to just realize I put out enough help or good into the world that I can ask for help without any strings."
Recommendation: Design intake and clinical interactions that explicitly normalize emotional and physical needs at multiple touchpoints and reduce reliance on self-advocacy.
Finding #1:
Strength Operates as a System constraint
Insight: Traditional patient-provider hierarchies decrease psychological safety. Shared racial or cultural identity between patients and providers increased trust, disclosure, and perceived care quality.
"That [racially concordant care] was important to me because when I walked into the room, I felt like... I was able to relate. I didn't worry about the judgment or the idea of malpractice that I have read about.
Recommendation: Train providers to recognize cultural power dynamics and use shared-decision framing during care interactions. Expand concordant care pathways, including doulas and midwives, as a core service design strategy-not an add-on.
Finding #2:
vulnerability is a design outcome
Insight: Mothers only expressed vulnerability when systems actively communicated safety and responsiveness.
"All the appointments were about baby. But they would always have me fill out those questionnaires... And I would fill it out really honestly, and saying, I need help. I am struggling. I am really sad. I'm really upset. I don't know why. I'm struggling, I need help. And I just felt like I didn't get that. I would get a call saying like, 'we saw that you filled this out and we're emailing you resources, or we're putting in a referral..' There was no additional follow-up.'
Recommendation: Replace passive follow-ups (e.g., emailed resources) with real-time, relational support pathways to create explicit signals that vulnerability is expected and supported.
Finding #3:
Racial concordance shifts power Dynamics
Insight: Racially and culturally concordant care allowed mothers to retain protective aspects of strength (resilience, determination) while also accessing support.
"A lot of things were understood without having to be explained completely... especially in terms of just feeling like I had to be super or not even just... I mean just a natural response to life. It allowed me to be a little softer and just relax and just accept people are here to help you.'
Recommendation: Reframe strength in system design by allowing resilience and vulnerability to coexist through flexible support pathways and adaptive care models.
Finding #4:
Resilience and vulnerability are not opposites
Lessons Learned
When systems feel unsafe, users change their behavior, not the system.
Users connect to services when they feel seen, respected, and emotionally safe.
Vulnerability emerges only when systems actively signal support, care, and follow-through.
Emotional safety should be treated as a fundamental usability metric, not optional.
Cultural narratives (like expectations of strength) shape behavior across touchpoints as much as interfaces.
Systems must be designed to surface, acknowledge, and address these constraints.
Personal Takeaways
How this study has changed my practice:
I now look for what users are compensating for, not just what they say they need
I treat emotional safety as a core usability metric, especially in high-stakes domains
I design research to surface power, identity, and context-not just workflows
Coming from a behavioral research background, l believe it is important to approach UX research beyond just user interfaces. Through this study, I learned that good UX isn't just about screens-it's about designing for the emotional and cultural realities of users. This project really shifted how I think about resilience-it's often a signal that the system just isn't doing enough.
From a UX research standpoint, this case shows how cultural narratives can function as hidden usability issues that shape behavior across an entire service ecosystem.